Drug-Induced Pneumonitis

By Leah Margolis Fingerman, NP, Interstitial Lung Disease Committee
Drug-induced pneumonitis refers to inflammation of the lung parenchyma caused by a medication. The onset can vary – median time to onset is 3 months, however there is a wide range (2-24 months) and can occur months after discontinuation.
Common Causes
- Immune checkpoint inhibitors (e.g., pembrolizumab, nivolumab) – The lungs have extensive immune capacity making them a common site of complications from immunotherapy.
- Bleomycin
- Methotrexate
- Amiodarone
- Nitrofurantoin
- Sulfonamides
- TNF-alpha inhibitors (Etanercept, Infliximab, Adalimumab)
- Certain anticonvulsants
Risk Factors
- Non Small Cell Lung Cancer (NSCLC) and Renal Cell Carcinomas (RCC) are associated with 2 to 3 fold higher incidence than melanoma
- One study indicates incidence in NSCLC could approach 20% for all grades
- Reduced risk seen in adenocarcinoma subtype of NSCLC, although mortality in this subgroup is higher
- Pre-existing ILD confers 6 to 10 fold increased risk
Clinical Presentation
- Dyspnea (most common)
- Dry cough
- Fatigue
- Low-grade fever
- Chest pain (less common)
- Hypoxemia (can be severe in advanced cases)
Up to 30% of patients are asymptomatic at presentation
Physical Exam
- Crackles (often bibasilar)
- May be normal early on
Radiographic Patterns
Imaging findings vary widely. Radiographic imaging patterns include any of the following patterns:
- Ground glass opacities
- Organizing pneumonia pattern
- NSIP-like pattern
- Hypersensitivity pneumonitis pattern
- Diffuse alveolar damage (severe cases)
Diagnosis:
There is no gold standard diagnostic test. The primary modality is imaging with a high resolution CT chest scan. It’s imperative to take a history with thorough medication review, rule out infectious causes, obtain a PFT with 6MWT/O2 titration, and consider bronchoscopy with BAL/TBBx.
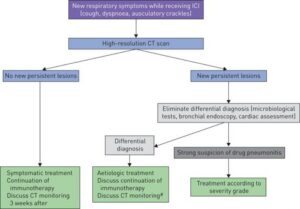
Delaunay et al., 2019 (European Respiratory Review)
Grading System for Diagnosis and Management:
Grade 1:
Asymptomatic, confined to one lobe of the lung or 25% of the lung parenchyma, clinical or diagnostic observations only
Management: Therapy can be continued with close monitored. Repeat CT chest scan in 3-4 weeks. If no improvement, treat as grade 2.
Grade 2:
Symptomatic and limiting ADLs, involves more than one lobe of the lung or 25-50% of lung parenchyma. Intervention is indicated.
Management: Hold drug, start prednisone 1 mg/kg/day and taper over ~6 weeks. Consider bronchoscopy.
Grade 3:
Severe symptoms, hypoxemic, hospitalization required. Involves all lung lobes or 50% of lung parenchyma
Management: Permanently stop drug, hospitalize patient. Start prednisone 1-2 mg/kg/day or IV methylprednisolone 1-2mg/kg/day. Steroids should be tapered over the course of 6-12 weeks. If symptoms do not improve within 48-72 hours of high dose steroids, infliximab may be offered
Grade 4:
Life threatening respiratory compromise, intubation may be indicated.
Management: Permanently stop drug, consider adding tocilizumab, mycophenolate, azathioprine, and/or IVIG
Case Example
66 y/o male with a history of basaloid squamous cell carcinoma presented with shortness of breath.
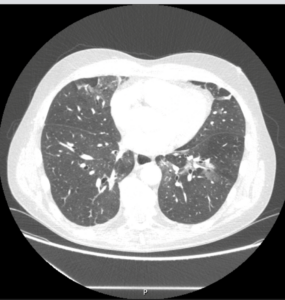
 In January 2025, he was started on an immunotherapy, Cemiplimab (Libtayo). In September 2025, during a routine scan, he was found to have “pneumonia” despite being asymptomatic at the time. Over time, he developed worsening respiratory symptoms, including difficulty breathing and a fever. Initial treatment with antibiotics was ineffective. It was later suspected that his symptoms were due to a drug reaction so he was started on prednisone with immediate relief in his symptoms.
In January 2025, he was started on an immunotherapy, Cemiplimab (Libtayo). In September 2025, during a routine scan, he was found to have “pneumonia” despite being asymptomatic at the time. Over time, he developed worsening respiratory symptoms, including difficulty breathing and a fever. Initial treatment with antibiotics was ineffective. It was later suspected that his symptoms were due to a drug reaction so he was started on prednisone with immediate relief in his symptoms.
After a six-week suspension of immunotherapy, he resumed treatment and experienced a recurrence of respiratory symptoms. Follow up CT chest scan showed worsening of the consolidation and groundglass opacities in bilateral lower lobes. The immunotherapy was held October 2025 and we did an 8 week prednisone taper at 0.5 mg/kg/day.
He was nearing completion of a course of prednisone in December 2025. Shortly after, he began experiencing symptoms such as productive cough, fever, and malaise. He was diagnosed with pneumonia and prescribed Levaquin with significant improvement in his symptoms. He is able to walk a mile and exercise without significant breathing difficulties.
 He has been off cemiplimab since October 2025 due to pneumonitis. We are monitoring his CT chest imaging closely every 3 months.
He has been off cemiplimab since October 2025 due to pneumonitis. We are monitoring his CT chest imaging closely every 3 months.
Leah Fingerman, NP
Sources
- Brahmer, J. R., Lacchetti, C., Thompson, J. A., et al. (2018). Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: American Society of Clinical Oncology clinical practice guideline summary.Journal of Oncology Practice, 14(4), 247–249.https://doi.org/10.1200/JOP.18.00005
- Cho JY, Kim J, Lee JS, Kim YJ, Kim SH, Lee YJ, Cho YJ, Yoon HI, Lee JH, Lee CT, Park JS. Characteristics, incidence, and risk factors of immune checkpoint inhibitor-related pneumonitis in patients with non-small cell lung cancer. Lung Cancer. 2018 Nov;125:150-156. doi: 10.1016/j.lungcan.2018.09.015. Epub 2018 Sep 18. PMID: 30429014.
- Delaunay, M., et al. (2019). Immune-checkpoint inhibitors associated with interstitial lung disease in cancer patients.European Respiratory Review, 28, 190012.https://doi.org/10.1183/16000617.0012-2019
- Delaunay M, Prévot G, Collot S, Guilleminault L, Didier A, Mazières J. Management of pulmonary toxicity associated with immune checkpoint inhibitors. Eur Respir Rev. 2019 Nov 6;28(154):190012. doi: 10.1183/16000617.0012-2019. PMID: 31694838; PMCID: PMC9488507.
- Medoff, B. D. (2025).[Pulmonary Complications][Lecture]. ILD Collaborative. https://www.ildcollaborative.org
- Naidoo, J., Wang, X., Woo, K. M., Iyriboz, T., Halpenny, D., Cunningham, J., Chaft, J. E., Segal, N. H., Callahan, M. K., Lesokhin, A. M., Rosenberg, J., Voss, M. H., Rudin, C. M., Rizvi, H., Hou, X., Rodriguez, K., Albano, M., Gordon, R. A., Leduc, C., … Hellmann, M. D. (2017). Pneumonitis in patients treated with anti–programmed death-1/programmed death ligand 1 therapy.Journal of Clinical Oncology, 35(7), 709–717.https://doi.org/10.1200/JCO.2016.68.2005
- Nishino, M., Chambers, E. S., Chong, C. R., Ramaiya, N. H., Gray, S. W., Marcoux, J. P., Hatabu, H., Hodi, F. S., & Awad, M. M. (2016). Anti–PD-1 inhibitor–related pneumonitis in non–small cell lung cancer.Clinical Cancer Research, 22(24), 6051–6060.https://doi.org/10.1158/1078-0432.CCR-16-1320
- Suresh, K., Voong, K. R., Shankar, B., Forde, P. M., Ettinger, D. S., Marrone, K. A., Kelly, R. J., Hann, C. L., Levy, B., Feliciano, J. L., Brahmer, J. R., Feller-Kopman, D., Lerner, A. D., Lee, H., Yarmus, L., D’Alessio, F., Hales, R. K., Lin, C. T., Psoter, K. J., … Naidoo, J. (2018). Pneumonitis in non-small cell lung cancer patients receiving immune checkpoint immunotherapy: Incidence and risk factors.Journal of Thoracic Oncology, 13(12), 1930–1939.https://doi.org/10.1016/j.jtho.2018.08.2035
